Blood Thinner Safety Comparison Tool
Find the Safest Blood Thinner for You
Answer a few questions about your health to see which DOAC (apixaban, rivaroxaban, or dabigatran) is safest for your specific situation.
Personalized Recommendation
When you're prescribed a blood thinner, the goal is simple: prevent clots without causing bleeding. But not all direct oral anticoagulants (DOACs) are the same. Apixaban, rivaroxaban, and dabigatran - three of the most common ones - may look similar on paper, but their side effect profiles are very different. Choosing the right one isn’t just about cost or dosing schedule. It’s about matching the drug to your body’s risks. And the data now makes it clear: one of these drugs is consistently safer for your stomach, another carries a hidden heart risk, and the third might be better for brain bleeding - even if it’s worse elsewhere.
Why This Matters More Than You Think
You’ve probably heard that DOACs are safer than warfarin. That’s true. But when you’re comparing apixaban, rivaroxaban, and dabigatran to each other, the differences aren’t small. They’re big enough to change your life. A 2022 study in JAMA Network Open tracked over 150,000 patients on these drugs. The results were startling. People taking rivaroxaban had more than double the risk of major bleeding compared to those on apixaban. Specifically, 39.7 major bleeds per 1,000 person-years for rivaroxaban versus just 18.5 for apixaban. That’s not a subtle difference - it’s the difference between needing a hospital visit every few years versus every year. And it’s not just about bleeding. One of these drugs is linked to more heart attacks. Another is harder on your kidneys. And one? It’s the only one that requires you to take it twice a day - no exceptions.Apixaban: The Gentlest on Your Stomach
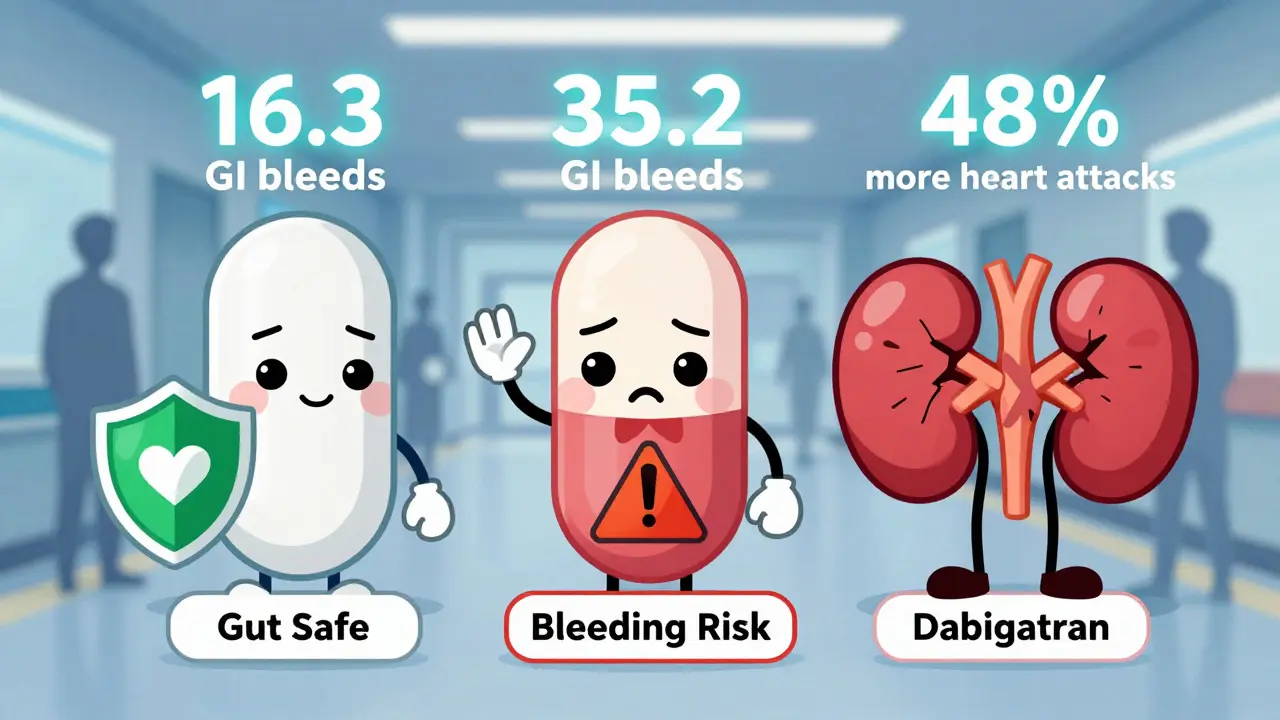
If you’ve ever had a stomach ulcer, take NSAIDs like ibuprofen regularly, or are over 75, apixaban might be your safest bet. Multiple large studies - including those from Oxford, JAMA, and the Annals of Internal Medicine - show apixaban causes significantly less gastrointestinal bleeding than the others. Here’s what the numbers say:- Apixaban: 16.3 GI bleeds per 1,000 person-years
- Rivaroxaban: 35.2 GI bleeds per 1,000 person-years
- Dabigatran: 32.2 GI bleeds per 1,000 person-years
Rivaroxaban: Once-Daily Convenience Comes at a Cost
Rivaroxaban’s biggest selling point is simplicity: one pill a day for stroke prevention. That helps with adherence. But that convenience hides a dangerous trade-off. While it has a lower rate of intracranial hemorrhage than apixaban (a 14% reduction, according to a 2022 study), it’s the worst offender when it comes to major bleeding overall. That includes bleeding in the abdomen, colon, and other internal organs. It’s also linked to higher total mortality - 44.2 deaths per 1,000 person-years compared to 41.0 for apixaban. That’s not a huge gap, but it’s consistent across studies. It’s also harder on the kidneys. About 33% of rivaroxaban leaves the body through the kidneys. That means if your kidney function drops below 15 mL/min, you can’t take it. For someone with moderate kidney disease, that rules out rivaroxaban entirely. And here’s the kicker: rivaroxaban is dosed twice daily when treating blood clots in the legs or lungs. So even though it’s marketed as a once-daily drug, many patients end up taking it twice a day - losing its main advantage.
Dabigatran: The Hidden Heart Risk
Dabigatran is the oldest DOAC. It works differently - it blocks thrombin, not factor Xa. That might sound like a technicality, but it has real consequences. First, it’s cleared almost entirely by the kidneys - 80%. That means if you have even mild kidney problems, you need a lower dose. The 150 mg dose is off-limits if your creatinine clearance is under 30 mL/min. The 110 mg dose? You can’t take it if it’s below 15 mL/min. But the bigger concern is your heart. Multiple meta-analyses - including one published in PMC and confirmed in JACC - show dabigatran increases the risk of heart attack and acute coronary syndrome by about 48% compared to rivaroxaban. Why? Researchers think it may trigger inflammation in blood vessels, similar to a drug (ximelagatran) that was pulled from the market for causing liver damage and heart issues. Dabigatran also has the highest rate of GI bleeding among the three. And because it’s taken twice daily, adherence can be a problem. No food restrictions help - but forgetting a dose means your protection drops faster than with the others.Which One Should You Take?
There’s no one-size-fits-all answer. But here’s how to think about it:- If you’ve had a stomach bleed, ulcers, or take NSAIDs → Choose apixaban. It’s the safest for your gut.
- If you have moderate kidney disease → Avoid dabigatran. Apixaban or rivaroxaban (if your kidneys are above 15 mL/min) are better.
- If you’re over 80 → Apixaban wins again. Lower bleeding risk, easier to manage.
- If you’re young, healthy, and want once-daily dosing → Rivaroxaban might work - but only if you have no history of GI issues or heart disease.
- If you’ve had a heart attack or have coronary artery disease → Avoid dabigatran. The data is too clear on the increased risk.
What About Cost and Availability?
All three are now available as generics. In the U.S., brand-name Eliquis (apixaban) costs around $518 for 60 tablets - but generics are far cheaper. GoodRx shows generic apixaban at under $20 per month in many cases. Rivaroxaban and dabigatran generics are similarly priced. So cost shouldn’t drive your choice. Safety should. Market data backs this up. Apixaban became the most prescribed DOAC in the U.S. by 2020 - and it’s still growing. Why? Because doctors are listening to the data. Patients aren’t just surviving - they’re bleeding less, hospitalizing less, and living longer.The Bottom Line
Apixaban, rivaroxaban, and dabigatran aren’t interchangeable. They’re three different tools - each with strengths and hidden dangers. - Apixaban: Best for your stomach, best for older adults, best overall safety profile. - Rivaroxaban: Convenient dosing, but highest risk of major bleeding and death. - Dabigatran: Highest kidney burden and the only one linked to more heart attacks. If you’re on one of these and haven’t discussed the risks with your doctor lately - do it now. Your next checkup might be the most important one you’ve had in years.Is apixaban really safer than the other DOACs?
Yes - for most people, especially those with kidney issues, older age, or a history of stomach bleeding. Multiple large studies, including JAMA 2022 and the Annals of Internal Medicine 2022, show apixaban causes significantly less gastrointestinal bleeding and major bleeding overall than rivaroxaban or dabigatran. It’s also the only DOAC with consistent safety data in patients over 80. While no drug is risk-free, apixaban has the most favorable safety profile across the board.
Why is dabigatran linked to more heart attacks?
Dabigatran directly inhibits thrombin, which plays a role in both clotting and inflammation. Studies suggest this inhibition may trigger a pro-inflammatory response in blood vessels, similar to what happened with ximelagatran - a drug withdrawn for causing heart attacks. Meta-analyses of five randomized trials show a 48% higher risk of heart attack or acute coronary syndrome with dabigatran compared to rivaroxaban. This risk appears consistent across different patient groups, even those without prior heart disease.
Can I switch from rivaroxaban to apixaban if I’m worried about bleeding?
Yes - and many doctors recommend it. If you’re on rivaroxaban and have risk factors like older age, kidney problems, or a history of stomach ulcers, switching to apixaban can significantly lower your bleeding risk. There’s no need to wait for a crisis. Talk to your doctor about your bleeding history, kidney function, and other medications. A simple switch can reduce your risk of hospitalization by up to 50% based on real-world data.
Does once-daily dosing really improve adherence?
It helps - but only if the dosing is truly once daily. Rivaroxaban is once daily for stroke prevention, but twice daily for treating clots in the legs or lungs. Many patients don’t realize this. Dabigatran is always twice daily. Apixaban is also twice daily. So if adherence is your main concern, the dosing schedule alone doesn’t make one drug better. What matters more is matching the drug to your lifestyle and health risks. For most, the safety benefits of apixaban outweigh the inconvenience of twice-daily dosing.
Are there any patients who should avoid apixaban?
Apixaban is safe for most people, but it’s not ideal if you have very severe kidney disease (creatinine clearance under 15 mL/min). It’s also not the best choice if you’re at high risk for intracranial bleeding - though this is rare. In very specific cases, like patients with mechanical heart valves, none of the DOACs are approved. Always check with your doctor. But for the vast majority - especially those over 65 or with GI risks - apixaban is the safest option available.












Post A Comment